Indications and Usage
GABITRIL (tiagabine hydrochloride) is indicated as adjunctive therapy in adults and children 12 years and older in the treatment of partial seizures.
Dosage and Administration
General:
The blood level of tiagabine obtained after a given dose depends on whether the patient also is receiving a drug that induces the metabolism of tiagabine. The presence of an inducer means that the attained blood level will be substantially reduced. Dosing should take the presence of concomitant medications into account.
GABITRIL (tiagabine HCl) is recommended as adjunctive therapy for the treatment of partial seizures in patients 12 years and older.
The following dosing recommendations apply to all patients taking GABITRIL:
- GABITRIL is given orally and should be taken with food.
- Do not use a loading dose of GABITRIL.
- Dose titration: Rapid escalation and/or large dose increments of GABITRIL should not be used.
- Missed dose(s): If the patient forgets to take the prescribed dose of GABITRIL at the scheduled time, the patient should not attempt to make up for the missed dose by increasing the next dose. If a patient has missed multiple doses, patient should refer back to his or her physician for possible re-titration as clinically indicated.
- Dosage adjustment of GABITRIL should be considered whenever a change in patient’s enzyme-inducing status occurs as a result of the addition, discontinuation, or dose change of the enzyme-inducing agent.
Induced Adults and Adolescents 12 Years or Older:
The following dosing recommendations apply to patients who are already taking enzyme-inducing antiepilepsy drugs (AEDs) (e.g., carbamazepine, phenytoin, primidone, and phenobarbital). Such patients are considered induced patients when administering GABITRIL.
In adolescents 12 to 18 years old, GABITRIL should be initiated at 4 mg once daily. Modification of concomitant antiepilepsy drugs is not necessary, unless clinically indicated. The total daily dose of GABITRIL may be increased by 4 mg at the beginning of Week 2. Thereafter, the total daily dose may be increased by 4 to 8 mg at weekly intervals until clinical response is achieved or up to 32 mg/day. The total daily dose should be given in divided doses two to four times daily. Doses above 32 mg/day have been tolerated in a small number of adolescent patients for a relatively short duration.
In adults, GABITRIL should be initiated at 4 mg once daily. Modification of concomitant antiepilepsy drugs is not necessary, unless clinically indicated. The total daily dose of GABITRIL may be increased by 4 to 8 mg at weekly intervals until clinical response is achieved or, up to 56 mg/day. The total daily dose should be given in divided doses two to four times daily. Doses above 56 mg/day have not been systematically evaluated in adequate and well-controlled clinical trials.
Experience is limited in patients taking total daily doses above 32 mg/day using twice daily dosing. A typical dosing titration regimen for patients taking enzyme-inducing AEDs (induced patients) is provided in Table 7.
Table 7: Typical Dosing Titration Regimen for Patients Already Taking Enzyme-Inducing AEDs
|
|
|
INITIATION AND TITRATION SCHEDULE |
|
TOTAL DAILY DOSE |
|
|
|
|
|
|
|
|
|
|
|
|
| WEEK 1 |
|
Initiate at 4 mg once daily |
|
4 mg / day |
|
|
|
|
|
|
| WEEK 2 |
|
Increase total daily dose by 4 mg |
|
8 mg / day (in two divided doses) |
|
|
|
|
|
|
| WEEK 3 |
|
Increase total daily dose by 4 mg |
|
12 mg / day (in three divided doses) |
|
|
|
|
|
|
| WEEK 4 |
|
Increase total daily dose by 4 mg |
|
16 mg / day (in two to four divided doses) |
|
|
|
|
|
|
| WEEK 5 |
|
Increase total daily dose by 4 to 8 mg |
|
20 to 24 mg / day (in two to four divided doses) |
|
|
|
|
|
|
| WEEK 6 |
|
Increase total daily dose by 4 to 8 mg |
|
24 to 32 mg / day (in two to four divided doses) |
32 to 56 mg / day in two to four divided doses
Non-Induced Adults and Adolescents 12 Years or Older:
The following dosing recommendations apply to patients who are taking only non-enzyme-inducing AEDs. Such patients are considered non-induced patients:
Following a given dose of GABITRIL, the estimated plasma concentration in the non-induced patients is more than twice that in patients receiving enzyme-inducing agents. Use in non-induced patients requires lower doses of GABITRIL. These patients may also require a slower titration of GABITRIL compared to that of induced patients (see CLINICAL PHARMACOLOGY, Pharmacokinetics and PRECAUTIONS, General, Use in Non-Induced Patients ).
Contraindications
GABITRIL is contraindicated in patients who have demonstrated hypersensitivity to the drug or its ingredients.
Adverse Reactions
The most commonly observed adverse events in placebo-controlled, parallel-group, add-on epilepsy trials associated with the use of GABITRIL in combination with other antiepilepsy drugs not seen at an equivalent frequency among placebo-treated patients were dizziness/light-headedness, asthenia/lack of energy, somnolence, nausea, nervousness/irritability, tremor, abdominal pain, and thinking abnormal/difficulty with concentration or attention.
Approximately 21% of the 2531 patients who received GABITRIL in clinical trials of epilepsy discontinued treatment because of an adverse event. The adverse events most commonly associated with discontinuation were dizziness (1.7%), somnolence (1.6%), depression (1.3%), confusion (1.1%), and asthenia (1.1%).
In Studies 1 and 2 (U.S. studies), the double-blind, placebo-controlled, parallel-group, add-on studies, the proportion of patients who discontinued treatment because of adverse events was 11% for the group treated with GABITRIL and 6% for the placebo group. The most common adverse events considered the primary reason for discontinuation were confusion (1.2%), somnolence (1.0%), and ataxia (1.0%).
Adverse Event Incidence in Controlled Clinical TrialsTable 5 lists treatment-emergent signs and symptoms that occurred in at least 1% of patients treated with GABITRIL for epilepsy participating in parallel-group, placebo-controlled trials and were numerically more common in the GABITRIL group. In these studies, either GABITRIL or placebo was added to the patient’s current antiepilepsy drug therapy. Adverse events were usually mild or moderate in intensity.
The prescriber should be aware that these figures, obtained when GABITRIL was added to concurrent antiepilepsy drug therapy, cannot be used to predict the frequency of adverse events in the course of usual medical practice when patient characteristics and other factors may differ from those prevailing during clinical studies. Similarly, the cited frequencies cannot be directly compared with figures obtained from other clinical investigations involving different treatments, uses, or investigators. An inspection of these frequencies, however, does provide the prescribing physician with one basis to estimate the relative contribution of drug and non-drug factors to the adverse event incidences in the population studied.
Table 5: Treatment-Emergent Adverse Event1 Incidence in Parallel-Group,
Placebo-Controlled, Add-On Trials (events in at least 1% of patients treated with GABITRIL and numerically more frequent than in the placebo group)
| Body System/COSTART |
|
GABITRIL N=494
|
|
Placebo N=275 |
|
|
|
% |
|
% |
| BODY AS A WHOLE |
|
|
|
|
| Abdominal Pain |
|
7 |
|
3 |
| Pain (unspecified) |
|
5 |
|
3 |
|
|
|
|
|
|
| CARDIOVASCULAR |
|
|
|
|
| Vasodilation |
|
2 |
|
1 |
|
|
|
|
|
|
| DIGESTIVE |
|
|
|
|
| Nausea |
|
11 |
|
9 |
| Diarrhea |
|
7 |
|
3 |
| Vomiting |
|
7 |
|
4 |
| Increased Appetite |
|
2 |
|
0 |
| Mouth Ulceration |
|
1 |
|
0 |
|
|
|
|
|
|
| MUSCULOSKELETAL |
|
|
|
|
| Myasthenia |
|
1 |
|
0 |
|
|
|
|
|
|
| NERVOUS SYSTEM |
|
|
|
|
| Dizziness |
|
27 |
|
15 |
| Asthenia |
|
20 |
|
14 |
| Somnolence |
|
18 |
|
15 |
| Nervousness |
|
10 |
|
3 |
| Tremor |
|
9 |
|
3 |
| Difficulty with Concentration/Attention* |
|
6 |
|
2 |
| Insomnia |
|
6 |
|
4 |
| Ataxia |
|
5 |
|
3 |
| Confusion |
|
5 |
|
3 |
| Speech Disorder |
|
4 |
|
2 |
| Difficulty with Memory* |
|
4 |
|
3 |
| Paresthesia |
|
4 |
|
2 |
| Depression |
|
3 |
|
1 |
| Emotional Lability |
|
3 |
|
2 |
| Abnormal Gait |
|
3 |
|
2 |
| Hostility |
|
2 |
|
1 |
| Nystagmus |
|
2 |
|
1 |
| Language Problems* |
|
2 |
|
0 |
| Agitation |
|
1 |
|
0 |
|
|
|
|
|
|
| RESPIRATORY SYSTEM |
|
|
|
|
| Pharyngitis |
|
7 |
|
4 |
| Cough Increased |
|
4 |
|
3 |
|
|
|
|
|
|
| SKIN AND APPENDAGES |
|
|
|
|
| Rash |
|
5 |
|
4 |
| Pruritus |
|
2 |
|
0 |
1Patients in these add-on studies were receiving one to three concomitant enzyme-inducing antiepilepsy drugs in addition to GABITRIL or placebo. Patients may have reported multiple adverse experiences; thus, patients may be included in more than one category.
*COSTART term substituted with a more clinically descriptive term.
Other events reported by 1% or more of patients treated with GABITRIL but equally or more frequent in the placebo group were: accidental injury, chest pain, constipation, flu syndrome, rhinitis, anorexia, back pain, dry mouth, flatulence, ecchymosis, twitching, fever, amblyopia, conjunctivitis, urinary tract infection, urinary frequency, infection, dyspepsia, gastroenteritis, nausea and vomiting, myalgia, diplopia, headache, anxiety, acne, sinusitis, and incoordination.
Study 1 was a dose-response study including doses of 32 mg and 56 mg. Table 6 shows adverse events reported at a rate of ≥ 5% in at least one GABITRIL group and more frequent than in the placebo group. Among these events, depression, tremor, nervousness, difficulty with concentration/attention, and perhaps asthenia exhibited a positive relationship to dose.
Drug Abuse and Dependence
The abuse and dependence potential of GABITRIL have not been evaluated in human studies.
Overdosage
Human Overdose Experience: Human experience of acute overdose with GABITRIL is limited. Eleven patients in clinical trials took single doses of GABITRIL up to 800 mg. All patients fully recovered, usually within one day. The most common symptoms reported after overdose included somnolence, impaired consciousness, agitation, confusion, speech difficulty, hostility, depression, weakness, and myoclonus. One patient who ingested a single dose of 400 mg experienced generalized tonic-clonic status epilepticus, which responded to intravenous phenobarbital.
From post-marketing experience, there have been no reports of fatal overdoses involving GABITRIL alone (doses up to 720 mg), although a number of patients required intubation and ventilatory support as part of the management of their status epilepticus. Overdoses involving multiple drugs, including GABITRIL, have resulted in fatal outcomes. Symptoms most often accompanying GABITRIL overdose, alone or in combination with other drugs, have included: seizures including status epilepticus in patients with and without underlying seizure disorders, nonconvulsive status epilepticus, coma, ataxia, confusion, somnolence, drowsiness, impaired speech, agitation, lethargy, myoclonus, spike wave stupor, tremors, disorientation, vomiting, hostility, and temporary paralysis. Respiratory depression was seen in a number of patients, including children, in the context of seizures.
Management of Overdose: There is no specific antidote for overdose with GABITRIL. If indicated, elimination of unabsorbed drug should be achieved by emesis or gastric lavage; usual precautions should be observed to maintain the airway. General supportive care of the patient is indicated including monitoring of vital signs and observation of clinical status of the patient. Since tiagabine is mostly metabolized by the liver and is highly protein bound, dialysis is unlikely to be beneficial. A Certified Poison Control Center should be consulted for up to date information on the management of overdose with GABITRIL.
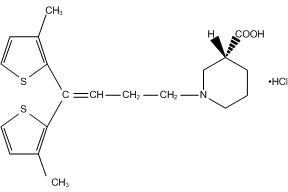
Description
GABITRIL® (tiagabine HCl) is an antiepilepsy drug available as 2 mg, 4 mg, 12 mg, and 16 mg tablets for oral administration. Its chemical name is (-)-(R)-1-[4,4-Bis(3-methyl-2-thienyl)-3-butenyl]nipecotic acid hydrochloride, its molecular formula is C20H25NO2S2 HCl, and its molecular weight is 412.0. Tiagabine HCl is a white to off-white, odorless, crystalline powder. It is insoluble in heptane, sparingly soluble in water, and soluble in aqueous base. The structural formula is:
GABITRIL tablets contain the following inactive ingredients: Ascorbic acid, colloidal silicon dioxide, crospovidone, hydrogenated vegetable oil wax, hydroxypropyl cellulose, hypromellose, lactose, magnesium stearate, microcrystalline cellulose, pregelatinized starch, stearic acid, and titanium dioxide.
In addition, individual tablets contain:
- 2 mg tablets: FD and C Yellow No. 6.
- 4 mg tablets: D and C Yellow No. 10.
- 12 mg tablets: D and C Yellow No. 10 and FD and C Blue No. 1.
- 16 mg tablets: FD and C Blue No. 2.
Clinical Pharmacology
Mechanism of Action
The precise mechanism by which tiagabine exerts its antiseizure effect is unknown, although it is believed to be related to its ability, documented in in vitro experiments, to enhance the activity of gamma aminobutyric acid (GABA), the major inhibitory neurotransmitter in the central nervous system. These experiments have shown that tiagabine binds to recognition sites associated with the GABA uptake carrier. It is thought that, by this action, tiagabine blocks GABA uptake into presynaptic neurons, permitting more GABA to be available for receptor binding on the surfaces of post-synaptic cells. Inhibition of GABA uptake has been shown for synaptosomes, neuronal cell cultures, and glial cell cultures. In rat-derived hippocampal slices, tiagabine has been shown to prolong GABA-mediated inhibitory post-synaptic potentials. Tiagabine increases the amount of GABA available in the extracellular space of the globus pallidus, ventral palladum, and substantia nigra in rats at the ED50 and ED85 doses for inhibition of pentylenetetrazol (PTZ)-induced tonic seizures. This suggests that tiagabine prevents the propagation of neural impulses that contribute to seizures by a GABA-ergic action.
Tiagabine has shown efficacy in several animal models of seizures. It is effective against the tonic phase of subcutaneous PTZ-induced seizures in mice and rats, seizures induced by the proconvulsant DMCM in mice, audiogenic seizures in genetically epilepsy-prone rats (GEPR), and amygdala-kindled seizures in rats. Tiagabine has little efficacy against maximal electroshock seizures in rats and is only partially effective against subcutaneous PTZ-induced clonic seizures in mice, picrotoxin-induced tonic seizures in the mouse, bicuculline-induced seizures in the rat, and photic seizures in photosensitive baboons. Tiagabine produces a biphasic dose-response curve against PTZ- and DMCM-induced convulsions, with attenuated effectiveness at higher doses.
Based on in vitro binding studies, tiagabine does not significantly inhibit the uptake of dopamine, norepinephrine, serotonin, glutamate, or choline and shows little or no binding to dopamine D1 and D2, muscarinic, serotonin 5HT1A, 5HT2, and 5HT3, beta-1 and 2 adrenergic, alpha-1 and alpha-2 adrenergic, histamine H2 and H3, adenosine A1 and A2, opiate µ and K1, NMDA glutamate, and GABAA receptors at 100 µM. It also lacks significant affinity for sodium or calcium channels. Tiagabine binds to histamine H1, serotonin 5HT1B, benzodiazepine, and chloride channel receptors at concentrations 20 to 400 times those inhibiting the uptake of GABA.
Pharmacokinetics
Tiagabine is well absorbed, with food slowing absorption rate but not altering the extent of absorption. The elimination half-life of tiagabine is 7 to 9 hours in normal volunteers. In epilepsy clinical trials, most patients were receiving hepatic enzyme-inducing agents (e.g., carbamazepine, phenytoin, primidone, and phenobarbital). The pharmacokinetic profile in induced patients is significantly different from the non-induced population (see PRECAUTIONS, General, Use in Non-Induced Patients ). The systemic clearance of tiagabine in induced patients is approximately 60% greater resulting in considerably lower plasma concentrations and an elimination half-life of 2 to 5 hours. Given this difference in clearance, the systemic exposure after a dose of 32 mg/day in an induced population is expected to be comparable to the systemic exposure after a dose of 12 mg/day in a non-induced population. Similarly, the systemic exposure after a dose of 56 mg/day in an induced population is expected to be comparable to the systemic exposure after a dose of 22 mg/day in a non-induced population.
Absorption and Distribution
Absorption of tiagabine is rapid, with peak plasma concentrations occurring at approximately 45 minutes following an oral dose in the fasting state. Tiagabine is nearly completely absorbed (>95%), with an absolute oral bioavailability of about 90%. A high fat meal decreases the rate (mean Tmax was prolonged to 2.5 hours, and mean Cmax was reduced by about 40%) but not the extent (AUC) of tiagabine absorption. In all clinical trials, tiagabine was given with meals.
The pharmacokinetics of tiagabine are linear over the single dose range of 2 to 24 mg. Following multiple dosing, steady state is achieved within 2 days.
Tiagabine is 96% bound to human plasma proteins, mainly to serum albumin and α1-acid glycoprotein over the concentration range of 10 ng/mL to 10,000 ng/mL. While the relationship between tiagabine plasma concentrations and clinical response is not currently understood, trough plasma concentrations observed in controlled clinical trials at doses from 30 to 56 mg/day ranged from less than 1 ng/mL to 234 ng/mL.
Metabolism and Elimination
Although the metabolism of tiagabine has not been fully elucidated, in vivo and in vitro studies suggest that at least two metabolic pathways for tiagabine have been identified in humans: 1) thiophene ring oxidation leading to the formation of 5-oxo-tiagabine; and 2) glucuronidation. The 5-oxo-tiagabine metabolite does not contribute to the pharmacologic activity of tiagabine.
Based on in vitro data, tiagabine is likely to be metabolized primarily by the 3A isoform subfamily of hepatic cytochrome P450 (CYP 3A), although contributions to the metabolism of tiagabine from CYP 1A2, CYP 2D6 or CYP 2C19 have not been excluded.
Approximately 2% of an oral dose of tiagabine is excreted unchanged, with 25% and 63% of the remaining dose excreted into the urine and feces, respectively, primarily as metabolites, at least 2 of which have not been identified. The mean systemic plasma clearance is 109 mL/min (CV = 23%) and the average elimination half-life for tiagabine in healthy subjects ranged from 7 to 9 hours. The elimination half-life decreased by 50 to 65% in hepatic enzyme-induced patients with epilepsy compared to uninduced patients with epilepsy.
A diurnal effect on the pharmacokinetics of tiagabine was observed. Mean steady-state Cminvalues were 40% lower in the evening than in the morning. Tiagabine steady-state AUC values were also found to be 15% lower following the evening tiagabine dose compared to the AUC following the morning dose.
Special Populations
Renal Insufficiency
The pharmacokinetics of total and unbound tiagabine were similar in subjects with normal renal function (creatinine clearance >80 mL/min) and in subjects with mild (creatinine clearance 40 to 80 mL/min), moderate (creatinine clearance 20 to 39 mL/min), or severe (creatinine clearance 5 to 19 mL/min) renal impairment. The pharmacokinetics of total and unbound tiagabine were also unaffected in subjects with renal failure requiring hemodialysis.
Hepatic Insufficiency
In patients with moderate hepatic impairment (Child-Pugh Class B), clearance of unbound tiagabine was reduced by about 60%. Patients with impaired liver function may require reduced initial and maintenance doses of tiagabine and/or longer dosing intervals compared to patients with normal hepatic function (see PRECAUTIONS ).
Geriatric
The pharmacokinetic profile of tiagabine was similar in healthy elderly and healthy young adults.
Pediatric
Tiagabine has not been investigated in adequate and well-controlled clinical trials in patients below the age of 12. The apparent clearance and volume of distribution of tiagabine per unit body surface area or per kg were fairly similar in 25 children (age: 3 to 10 years) and in adults taking enzyme-inducing antiepilepsy drugs ([AEDs] e.g., carbamazepine or phenytoin). In children who were taking a non-inducing AED (e.g., valproate), the clearance of tiagabine based upon body weight and body surface area was 2 and 1.5-fold higher, respectively, than in non-induced adults with epilepsy.
Gender, Race and Cigarette Smoking
No specific pharmacokinetic studies were conducted to investigate the effect of gender, race and cigarette smoking on the disposition of tiagabine. Retrospective pharmacokinetic analyses, however, suggest that there is no clinically important difference between the clearance of tiagabine in males and females, when adjusted for body weight. Population pharmacokinetic analyses indicated that tiagabine clearance values were not significantly different in Caucasian (N=463), Black (N=23), or Hispanic (N=17) patients with epilepsy, and that tiagabine clearance values were not significantly affected by tobacco use.
Interactions with other Antiepilepsy Drugs
The clearance of tiagabine is affected by the co-administration of hepatic enzyme-inducing antiepilepsy drugs. Tiagabine is eliminated more rapidly in patients who have been taking hepatic enzyme-inducing drugs, e.g., carbamazepine, phenytoin, primidone and phenobarbital than in patients not receiving such treatment (see PRECAUTIONS, Drug Interactions ).
Interactions with Other Drugs
See PRECAUTIONS, Drug Interactions.
Clinical Studies
The effectiveness of GABITRIL as adjunctive therapy (added to other antiepilepsy drugs) was examined in three multi-center, double-blind, placebo-controlled, parallel-group, clinical trials in 769 patients with refractory partial seizures who were taking at least one hepatic enzyme-inducing antiepilepsy drug (AED), and two placebo-controlled cross-over studies in 90 patients. In the parallel-group trials, patients had a history of at least six complex partial seizures (Study 1 and Study 2, U.S. studies), or six partial seizures of any type (Study 3, European study), occurring alone or in combination with any other seizure type within the 8-week period preceding the first study visit in spite of receiving one or more AEDs at therapeutic concentrations.
In the first two studies, the primary protocol-specified outcome measure was the median reduction from baseline in the 4-week complex partial seizure (CPS) rates during treatment. In the third study, the protocol-specified primary outcome measure was the proportion of patients achieving a 50% or greater reduction from baseline in the 4-week seizure rate of all partial seizures during treatment. The results given below include data for complex partial seizures and all partial seizures for the intent-to-treat population (all patients who received at least one dose of treatment and at least one seizure evaluation) in each study.
Study 1 was a double-blind, placebo-controlled, parallel-group trial comparing GABITRIL 16 mg/day, GABITRIL 32 mg/day, GABITRIL 56 mg/day, and placebo. Study drug was given as a four times a day regimen. After a prospective Baseline Phase of 12 weeks, patients were randomized to one of the four treatment groups described above. The 16-week Treatment Phase consisted of a 4-week Titration Period, followed by a 12-week Fixed-Dose Period, during which concomitant AED doses were held constant. The primary outcome was assessed for the combined 32 and 56 mg/day groups compared to placebo.
Study 2 was a double-blind, placebo-controlled, parallel-group trial consisting of an 8-week Baseline Phase and a 12-week Treatment Phase, the first 4 weeks of which constituted a Titration Period and the last 8 weeks a Fixed-Dose Period. This study compared GABITRIL 16 mg BID and 8 mg QID to placebo. The protocol-specified primary outcome measure was assessed separately for each group treated with GABITRIL.
The following tables display the results of the analyses of these two trials.
Table 1: Median Reduction and Median Percent Reduction from Baseline in 4-Week Seizure Rates in Study 1
|
|
|
Placebo (N=91) | GABITRIL 16 mg/day (N=61) | GABITRIL 32 mg/day (N=87) | GABITRIL 56mg/day (N=56) | Combined 32 and 56 mg/day (N=143) |
|
|
|
|
|
|
|
|
| Complex Partial | Median Reduction | 0.6 | 0.8 | 2.2 * | 2.9 * | 2.6 * |
|
|
Median % Reduction † | 9% | 13% | 25% | 32% | 29% |
|
|
|
|
|
|
|
|
| All Partial | Median Reduction | 0.2 | 1.2 | 2.7 * | 3.5 * | 2.9 * |
|
|
Median % Reduction † | 3% | 12% | 24% | 36% | 27% |
* p less than 0.05
† Statistical significance was not assessed for median % reduction.
Table 2: Median Reduction and Median Percent Reduction from Baseline in 4-Week Seizure Rates in Study 2
|
|
Placebo (N=107) | GABITRIL 16 mg BID (N=106) | GABITRIL 8 mg QID (N=104) | |
|
|
|
|
|
|
| Complex Partial | Median Reduction | 0.3 | 1.6 | 1.3 * |
|
|
Median % Reduction† | 4% | 22% | 15% |
|
|
|
|
|
|
| All Partial | Median Reduction | 0.5 | 1.6 | 1.3 |
|
|
Median % Reduction† | 5% | 19% | 13% |
* p less than 0.027 necessary for statistical significance due to multiple comparisons.
† Statistical significance was not assessed for median % reduction.
How Supplied / Storage and Handling
GABITRIL tablets are available in four dosage strengths.
2 mg orange-peach, round tablets, debossed with

4 mg yellow, round tablets, debossed with
12 mg green, ovaloid tablets, debossed with
16 mg blue, ovaloid tablets, debossed with
Recommended Storage: Store tablets at controlled room temperature, between 20-25°C (68-77°F). See USP. Protect from light and moisture.
Logo